Influenza & COVID-19

Influenza
Every year we eagerly await the 'flu letter' so we know what we are doing in the coming season.
The ‘flu letter’ with the intentions for the 25/26 season arrived 13th February 2025 (and advice for 26/27 was also trickling though). The 26/27 flu letter arrived 26/2/26.
We began the 25/26 vaccine clinics from 1st Sept for the kids and pregnant ladies, and 1st Oct on the adult and clinical risk groups 18+. This season and 24/25 are the only years we have staggered the starts and this is due to quicker waning immunity on older adults than in youngsters. An extra month to wait means the vaccine protection will carry through to the end of flu season. 26/27 will remain the same.
It's a massive undertaking to deliver the flu programme. And vaccine uptake across all groups has consistently droped since COVID-19 times. As of 23rd October 2025 we had vaccinated over 10.4 million (10,436,395) people against flu and almost three million (2,987,313) people against COVID. Well done all!! As of 8th Jan 2026 over 18.6 million eligible people were vaccinated. With flu still circulating please continue to do all you can to encourage eligible people to have their vaccine.
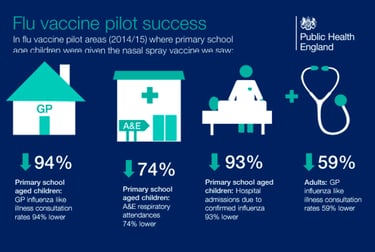
UKHSA published modelling estimates which suggested that flu vaccination had prevented approximately 100,000 hospitalisations in the 24/25 season in England
We hit the 25/26 flu season five weeks earlier than usual. Australia experienced a severe winter; France and Japan also reported very high activity. There was a mutated A strain in the summer which is always a risk when deciding on vaccine strains so far in advance. Hence, 25/26 has been a VERY challenging season. Fortunately the 25/26 vaccines have maintained their effectiveness.
QUICK CHANGES-FROM-LAST-YEAR NEWS!
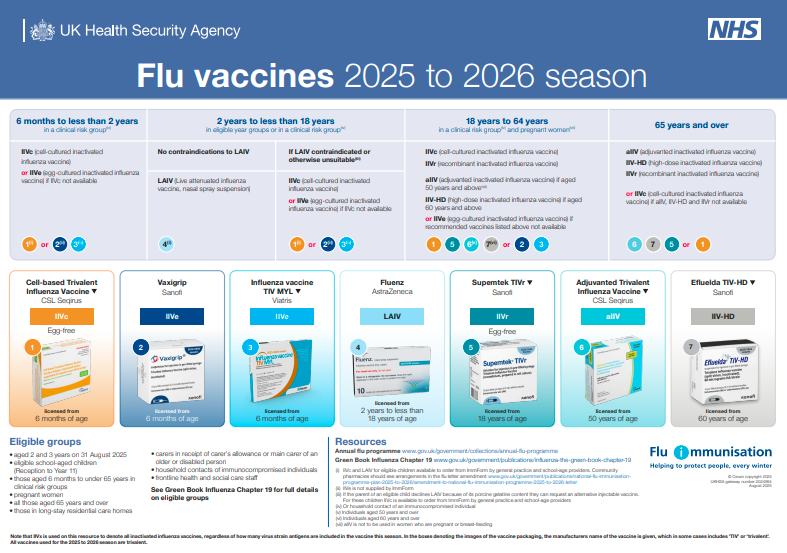
Previous years have seen quadrivalent vaccines (4 strains) but 25/26 said goodbye to the Yamagata B strain (due to not circulating for a while) and all UK vaccines are now trivalent.
In 25/26 aTIV became licenced from 50 years (TIVHD (60+)
TIVr made a return in 25/26!
LAIV now includes PGD provision for up to 25y in SEN schools.
Community pharmacy getting involved with 2/3y olds.
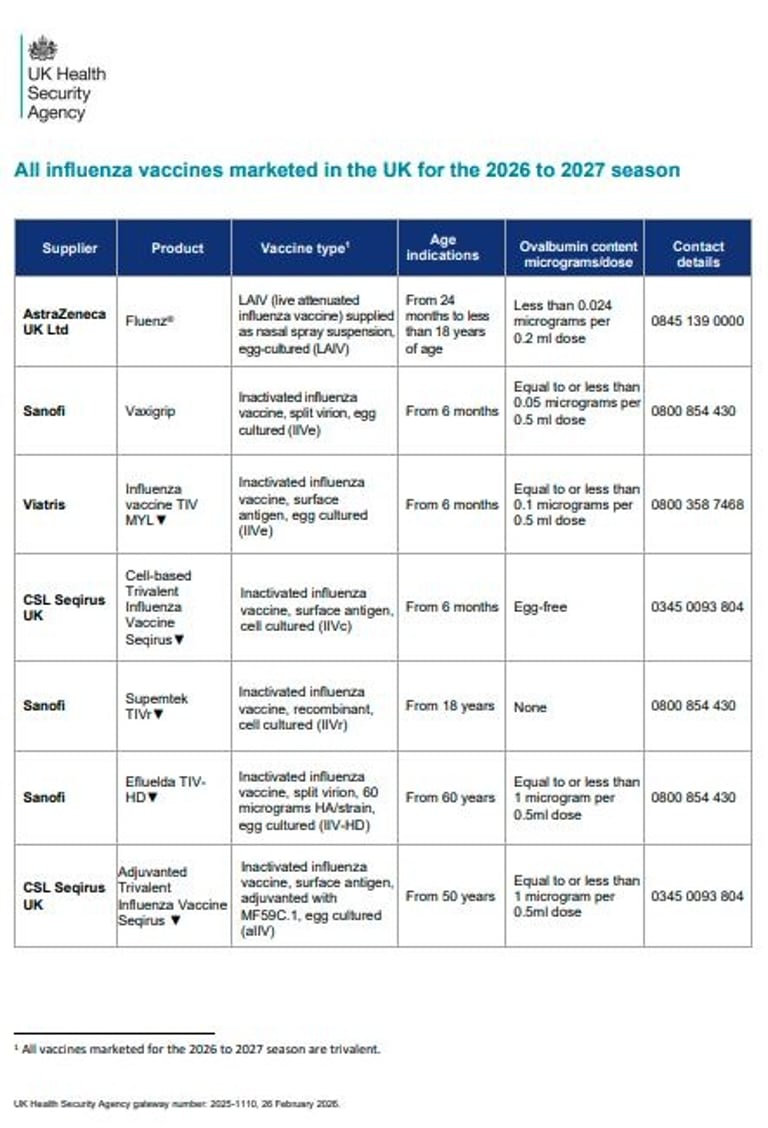
There are no changes to eligible cohorts for the 26/27 programme and the timing remains the same staggered (for some) start as last year.
There are some firm words in the flu letter about planning to do more for uptake in 26/27, especially in undeserved groups. The new GP contract aims to address these inequalities more fairly.
JCVI also advise prioritising 2/3 year olds for 26/27.
There have been 2 changes to the JCVI advice for adult flu vaccines for 2026 to 2027. Firstly, in those aged 65 years and older, IIVc should be considered equivalent to allV, llV-HD, and IIVr. And secondly, in those aged 50 years to 59 years in clinical risk groups, IIV-HD can be used off-label. Looking at the vaccines table, IIVe seems to be very much taking a back seat now.
Quick tip: When providing patients with details of the vaccine, it is good practice to give them details of the brand and batch number. This will allow patients and carers to more accurately report suspected ADRs to the Yellow Card scheme.
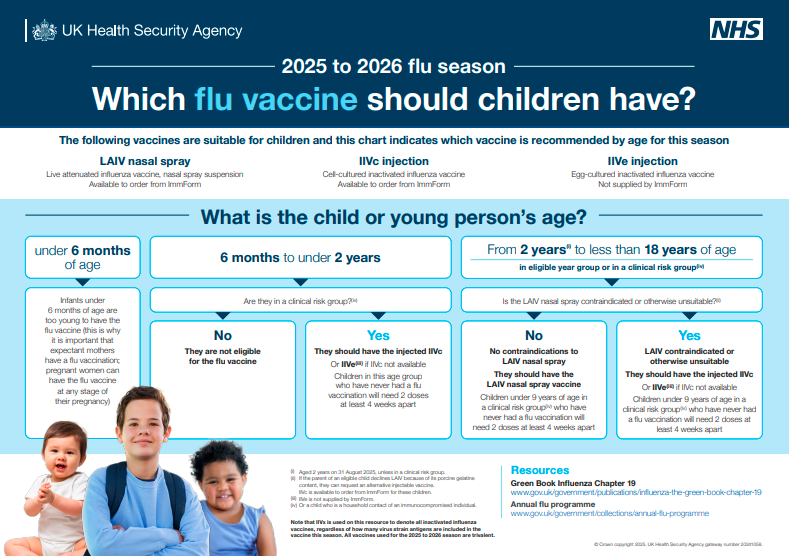

• LAIV is different from other flu vaccines – it is a live attenuated nasal vaccine and must not be injected
• Do not attempt to attach a needle
• Fluenz can be administered at the same time as, or at any interval from other vaccines including live vaccines
• Patient should breathe normally - no need to actively inhale or sniff
• The vaccine is rapidly absorbed so no need to repeat either half of dose if patient sneezes, blows their nose or their nose drips following administration
Administration of Nasal Flu Vaccine

IM administration
Note she doesn’t actually insert the needle in this demo (don’t forget to put it in!!!)



Results: "Access was NOT the primary issue underlying suboptimal vaccine uptake among participants in clinical risk groups, who instead cited low-risk perceptions of influenza infection and deficits of information about the relevance of vaccination for their condition management. Healthcare providers in non-primary care settings rarely discussed or recommended influenza vaccination across patient pathways, despite being able to address the concerns raised by participants in clinical risk groups." (I.E. vaccine uptake is not just about putting on the late night and weekend clinics! People may well make more efforts to show up if they knew WHY they should)
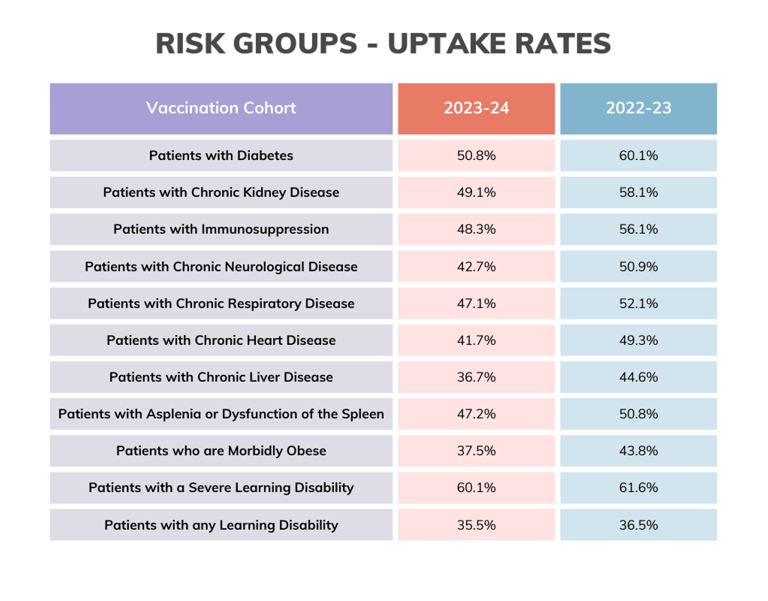
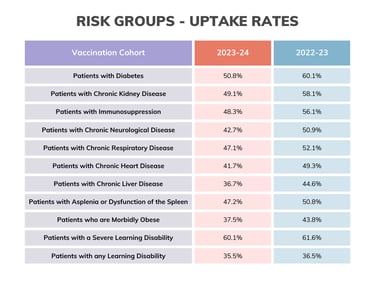

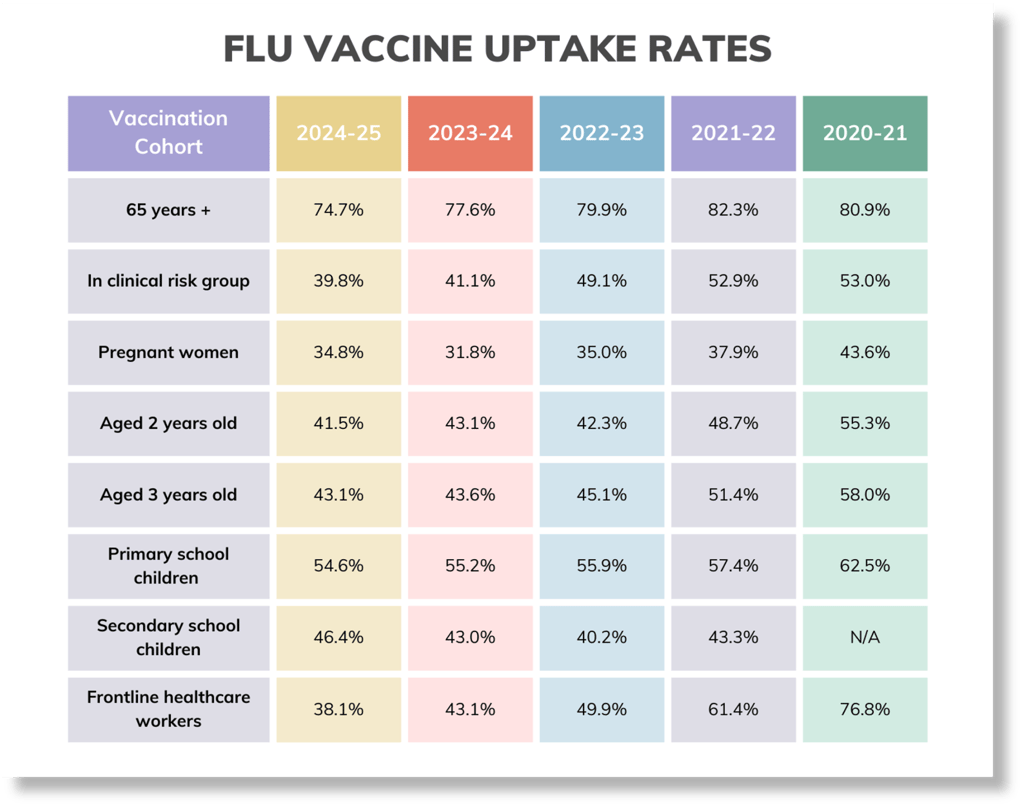
Uptake data to 31st Jan 2026
Here's a quick vaccine uptake snapshot as of data published 26th Feb:
A total of 45.4% of all frontline healthcare workers have been vaccinated for influenza (485,398 of 1,069,606).
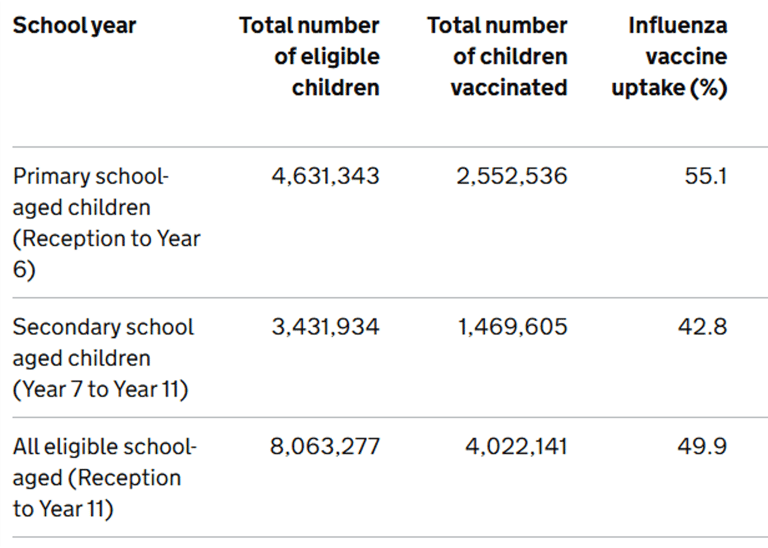
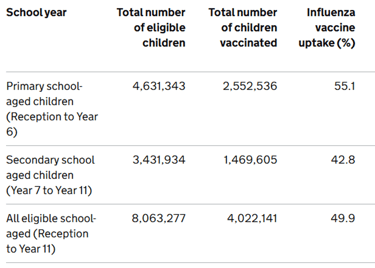
For children, the reception years are doing the best at 56.3%, with the age 2's and year 11's achieving the lowest uptake at 43.4%.
And for GP patients, over 65's are at 74.4%, under 65's in clinical risk groups are at 40.6% (worrying), pregnant women are at 38.5% (also worrying).
Flu vaccination in adult social care settings
Within the 99.1% of older adult care home providers who had updated their seasonal vaccination data as of 16 February 2026:
11.3% of total staff are known to have received a flu vaccination for the 2025 to 2026 season
66.7% of total residents are known to have received a flu vaccination for the 2025 to 2026 season
Within the 99.0% of younger adult care home providers who had updated their seasonal vaccination data as of 16 February 2026:
9.1% of total staff are known to have received a flu vaccination for the 2025 to 2026 season
54.5% of total residents are known to have received a flu vaccination for the 2025 to 2026 season

Arrived 3rd September 2025
Reflection points:
Do you know your local uptake figures?
In YOUR clinic, which are the most difficult groups to reach? Why?
Do you see similar results to the national figures?
What other vaccines might these groups be missing out on?

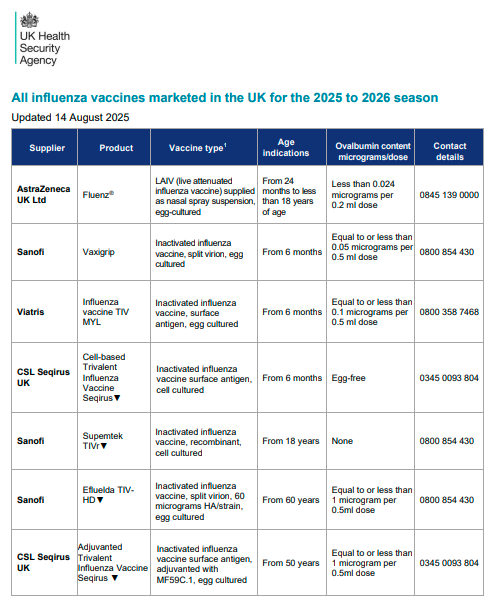
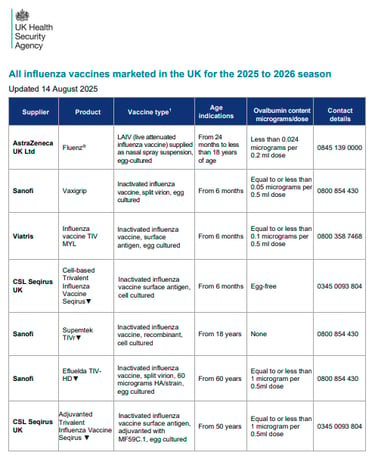
Ovalbumin content
LESS THAN 0.12MCG/ML = SAFE TO VACCINATE
(equivalent to <0.06mcg for 0.5ml dose)
Porcine Gelatine Content
Fluenz Tetra contains a small amount of highly purified porcine gelatine. This vaccine is the most effective option for children aged 2 and older but there is the injectable alternative if required.
Think about how these conversations are had....
Other queries about vaccine contents... Dogs, sharks and moths?
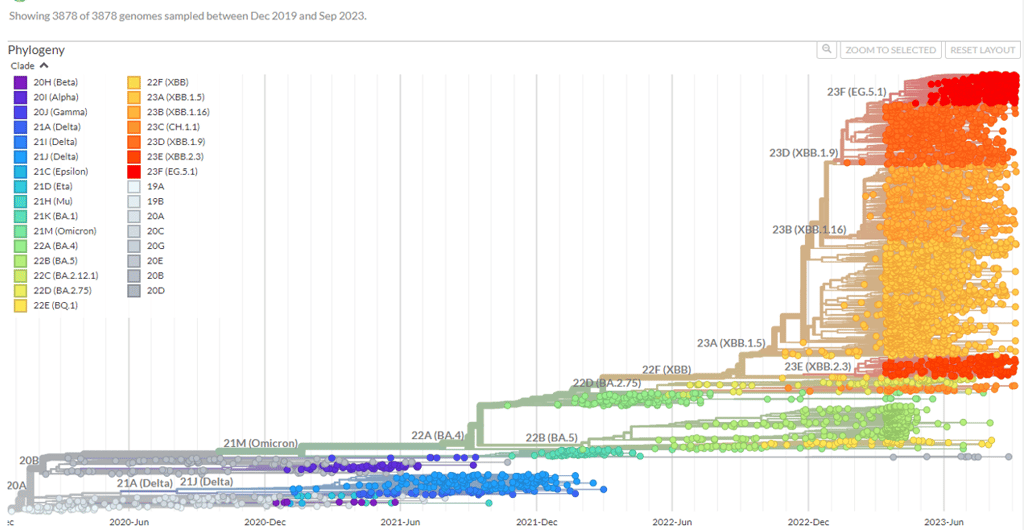
Why the need for boosters? New vaccines?Antigenic Drift and Shift: How the Influenza Virus Adapts










COVID-19
At least 15–20 million lives saved globally in the first year alone—and many more since—according to the modelling.
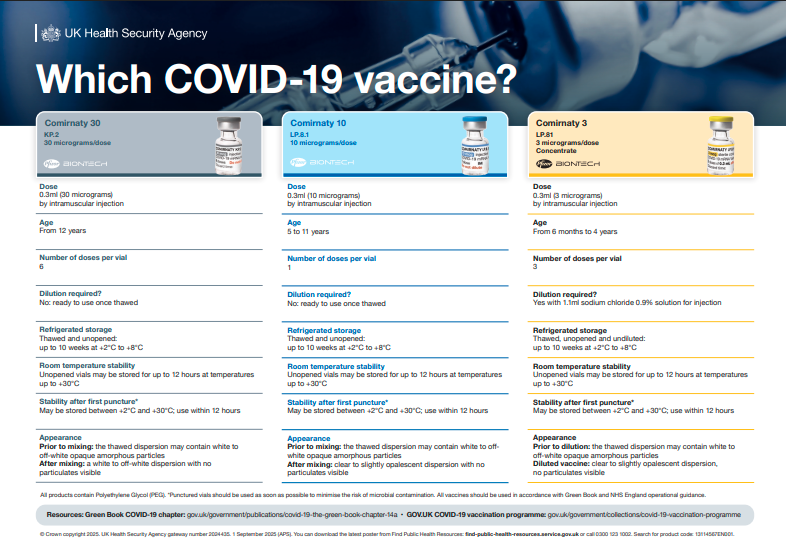
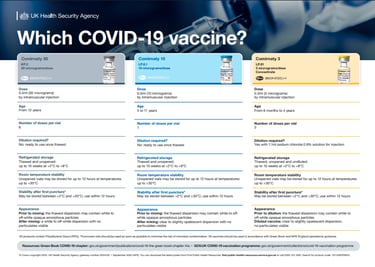
Autumn 2025 booster programme was 1st Oct-31st Jan, Check out the latest variant vaccines (and the helpful poster). Plenty of ongoing research (boosters & new variants). Hundreds of vaccines in development.
Eligibility adapting to context. Eligibility is narrowing - now 75+, care home residents and IC 6m+.
Check out this headline: Pharmacies facing angry patients over Covid jab confusion.
Could COVID-19 move to an all year round prog? JCVI minutes from June indicate it's up for consideration.
Vaccines evolving – bivalent options, new variants, nasal options? Combined vaccines? Where is the 2 in 1 COVID and flu jab up to? Could this be with us in 2026?
Legal changes have lead to some confusion and misunderstandings with other vaccines - check your legal mechanisms!
Pandemic disruption has left much catching up to do with other vaccines




If you want to REALLY geek out try this website...